Fill-finish is a critical part of biopharmaceutical manufacture, any mistakes at this point can lead to the product being incorrectly formulated, contaminated, or improperly packaged which in turn leads to safety issues, production failures and ultimately, the loss of viable product just as it advances to its most valuable point of production.
At this stage of manufacture, robust, trusted processes are required to manage any risk to operations.
Operator involvement is closely tied with sterility assurance. The more involved operators are in the filling process, the more likely sterility assurance failures may occur. While operator involvement is sometimes necessary, it, unfortunately, creates a larger risk of contamination. Isolator-based filling removes operators from the filling environment thereby decreasing opportunities for sterility assurance failures. The increased sterility assurance offered by isolators is the reason why they are preferred in the drug production process.
This article explores the development of isolator-based filling systems and the improvements in technology over the last few decades, the introduction of robotics and technology and presents a case study for the optimal solution for sterile, isolator-based filling.
Early isolator filling
In the early 80’s isolators first started to appear in the pharmaceutical industry and were primarily deployed in sterility testing. Like any new technology, the isolators were clumsy and awkward at first, with some significant weaknesses. Despite their ability to effectively sterilize, they were very expensive relative to traditional cleanrooms. They also had long sanitization and aeration times, they were not very ergonomic for the operators and they were very inflexible as each system was designed for very specific activities.
For a long time, small-batch fill-finish CMOs accommodated different container types and sizes with separate filling lines for each. This was very expensive in terms of equipment and cleanroom requirements as a different filling line was necessary for each type of container. With this being the case, most small CMOs chose to concentrate on only one type of container, the vial.
Improvements in technology
As isolators were making their way into sterile manufacturing, ready-to-use (RTU) pre-filled syringes with nested plungers increased in popularity. Eventually, RTU syringes and isolator-based filling were combined. Soon other glass container manufacturers realized that it was possible to place other containers (vials and cartridges) in similar nested formats for filling on these XY fillers. Thus, began the RTU vial and cartridge line.
XY fillers were adapted to fill multiple RTU nested containers, which increased the flexibility of the filling line, but there were limited choices for nested RTU vials and cartridges available. Bulk glass vial lines were, and still are, very popular as there is a perception that bulk vials, which need to be washed and depyrogenated, are considerably less expensive than RTU vials. This resulted in fill-finish CMOs focusing primarily on either RTU containers or bulk vials, somewhat limiting a client’s choice in container type.
Early isolator-based filling lines were not designed to be flexible. They were also large and required a lot of cleanroom space. These filling lines were and still are considerably more expensive and complex than the traditional cleanroom. Despite isolators providing greatly improved sterility assurance over restricted access barriers (RABS), the cost, inflexibility, and other shortcomings prevented many small-batch fill-finish companies from adopting this technology.
Introduction of flexible isolators for small scale use
Small-scale fill-finish CMOs that manufacture products for pre-clinical, clinical, or small commercial use were the last to adopt isolator-based filling. Most of these drug products were new treatments that did not have a fully vetted manufacturing process. Interventions at this scale are often necessary to continue a fill, so access to the sterile core of the filling line is a priority for these CMOs. Furthermore, these companies typically had multiple filling lines dedicated to each container type. The cost to upgrade these to isolator-based lines dissuaded many small-batch CMOs from investing in isolators.
The need for a flexible, isolator-based filling line was high. In 2016, Berkshire Sterile Manufacturing’s semi-automated filling line began operation (now Sharp Sterile Manufacturing, Berkshire Sterile Manufacturing was acquired by Sharp in 2023). This line was one of the first small-scale filling lines with the flexibility to fill syringes, cartridges, vials (either RTU or bulk), and lyophilized product all on the same filling line. The line was also 100% isolator-based.
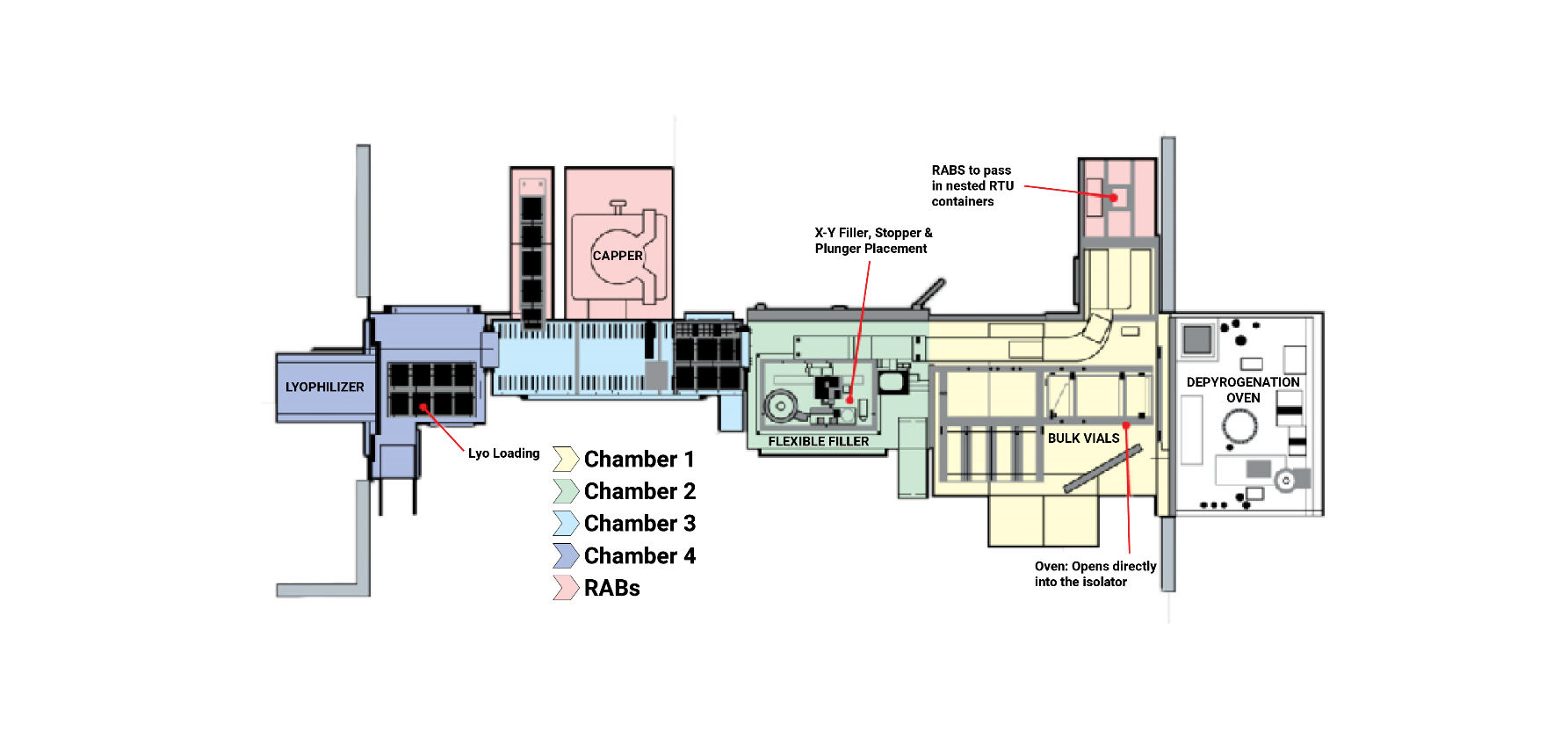
Figure 1. Layout of BSM’s semi-automated filling line. The isolator-based filling line was designed to process RTU syringes, vials, and cartridges, bulk vials, and lyophilized product.
The company worked with four major equipment suppliers – Colanar, IMA, Genesis, and Steriline – to develop a customized isolator line containing two separate entrances for RTU containers and bulk vials, a fully flexible, XY filler, and a diverting chamber that would lead syringes and cartridges out an exit RABS and vials to and from the lyophilizer and out a capper based in a RABS.
This line was designed to fill up to 40,000 units of drug product per lot and offered a piston pump option for high viscosity fills. All areas of the isolator are accessible by operators through the use of glove ports, so if an intervention is required, the operator can perform any necessary corrective action.
The introduction of this line prompted many other CMOs to build their own flexible and isolator-based filling lines, and today, isolator-based filling is the expectation.

BSM’s semi-automated isolator-based filling line (pictured) was one of the first small scale filling lines capable of filling multiple container types and sizes in an isolated environment. (Photo owned by BSM).
Introduction of robotics/automation
Sterile filling can still be improved by reducing operator involvement in the filling process where possible. Though filling lines have been improved by basing them in isolators, operators are still required to aid in the filling process by performing actions through glove ports in the isolators. For example, operators may be used to load and unload the fillers, transport materials into and out of the filling line, and denest vials into a capper or push filled syringes and cartridges out of a RABS exit. Any action performed by an operator adds risk. Many equipment suppliers offer automated systems for transporting containers, filling and stoppering, and capping (for vial fills).
These advancements in technology have allowed companies who focus on large scale production to remove operators from their filling process, and thus dramatically improve the sterility assurance and quality of the products they produce; however, small-scale companies have not been as keen to this change. Small-scale fill-finish CMOs face a similar trade-off as they once did with isolators: if they adopt this new technology (automation and robotics), they will lose on flexibility.
Automated systems are great for performing a single action in repetition. As a result, the automated filling lines we see today are built to fill only one container type: vials, syringes, or cartridges. Furthermore, automated filling lines for vials may only fill bulk vials or only RTU vials.
The cost to build several dedicated, isolator-based, and fully automated filling lines for each container type is prohibitive. Again, small-scale fill-finish companies are often hesitant to embrace automation in filling because of the cost, perceived inflexibility, and other shortcomings.
The solution
The solution is a newly designed fully automated, isolator-based system offering the same flexibility as a semi-automated filling line. Developed by Berkshire Sterile Manufacturing in collaboration with several companies including Steriline, Colanar, IMA, and Genesis, it has the potential to redefine small-scale manufacturing.
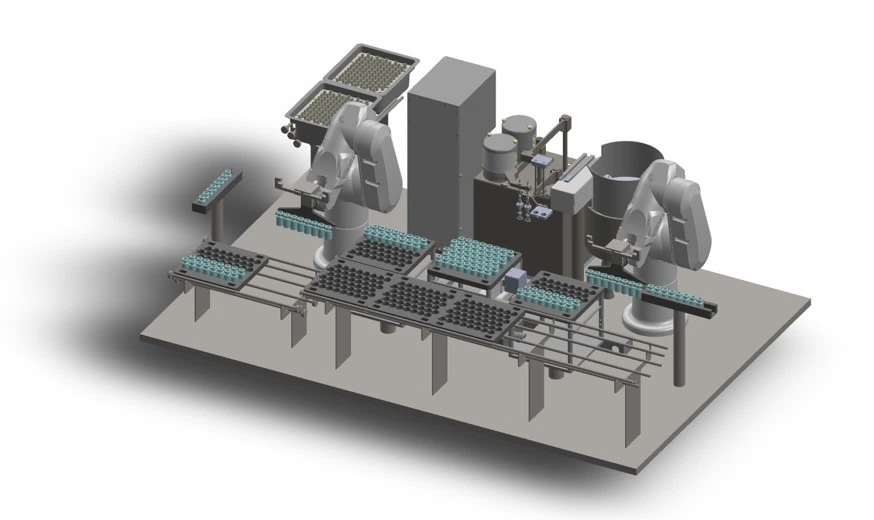
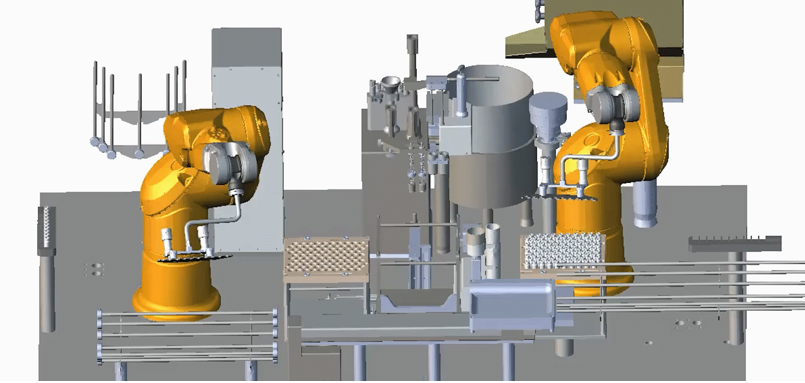
The design of the filling line is centered on an isolator-based, ultra-flexible and fully automated Colanar filler, capable of filling vials, syringes, and cartridges of different sizes. On each side of this flexible filler are two advanced Staubli robotic arms that will load and unload the filler. The line will also have lyophilization capability.
There are two entrances to this filling isolator: one for RTU containers, and another for bulk vials. RTU containers will be introduced into the filling isolator in their tubs allowing the first robot arm to easily pick up the nest and place it on the XY filler.
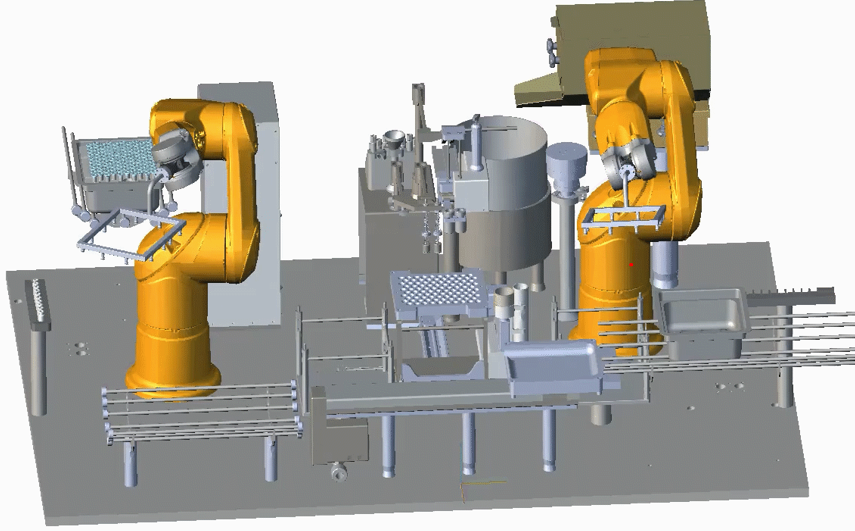
Pictured: The two robotic arms will load and unload the flexible filler with nested containers. (Simulation created by Colanar)
Bulk vials, on the other hand, will be processed in a depyrogenation tunnel before entering the filling isolator. The vials will be presented off a conveyor belt, and the first robotic arm will pick up these vials and load them into a nest. Once the nest is full, the robot will place the nest onto the filler to be filled and stoppered.
Syringes and cartridges will exit the filling line through an exit RABS attached directly to the filling isolator. Vials (either RTU or bulk) will be denested onto a conveyor belt that will automatically divert them to an IMA lyophilizer or to a medium speed Genesis capper based in a RABS.
This system will provide a fully automated and highly flexible solution for small batch sterile filling. The line will also feature several new technologies, including a new online technique for 100% in-process checks that are real-time and do not slow down production speed.
It’s expected that necessary interventions will arise during some fills. To further reduce operator involvement, the isolator line will be equipped with several vision systems from Cognex. These systems will observe the activity in the isolator, identify errors, and report to the robotic arms the necessary recovery steps they will need to take to restore the system to working order. As a last resort, BSM chose to include glove ports on the isolator to allow operators to intervene in case of unforeseen issues.
This approach offers a lot of flexibility. This system can fill all popular container types and sizes. This filling system could also use a peristaltic pump or a piston pump to fill viscous products.
Conclusion
Isolator-based filling technology removes the risk of human contamination from the formulation and filling process. Technological improvements and the adoption of robotics and automated processes have steadily increased sterility assurance and have become more flexible over recent years. Ultimately, more robust and efficient isolator-based fill-finish lines raise the standard for sterility assurance and de-risk development and manufacturing for very high-value products.
Sharp offers clients a seamless, end-to-end pharmaceutical manufacturing, packaging and distribution solution specifically aimed at small-batch syringes, vials and cartridges. Get in touch to learn how our combined expertise can work for you.